WHAT IS ILIOTIBIAL BAND (ITB) SYNDROME?
Iliotibial band (ITB) syndrome is the most common cause of outer knee pain among athletes. (M. Fredericson. Practical Management of Iliotibial Band Friction Syndrome in Runners. Clin J Sport Med: May 2006 - Vol 16 (3) p 261-8) It develops as a non-traumatic, gradual increase of pain that is within the category of overuse syndromes/injuries. This condition is usually seen in runners and cyclists, but athletes of other sports can be affected as well. In ITB syndrome, pain in the outer knee is felt with foot contact in runners and as the knee extends (straightens) in cyclists. ITB syndrome is also seen in athletes who participate in tennis, soccer, volleyball, and skiing.
ANATOMY OF THE IT BAND
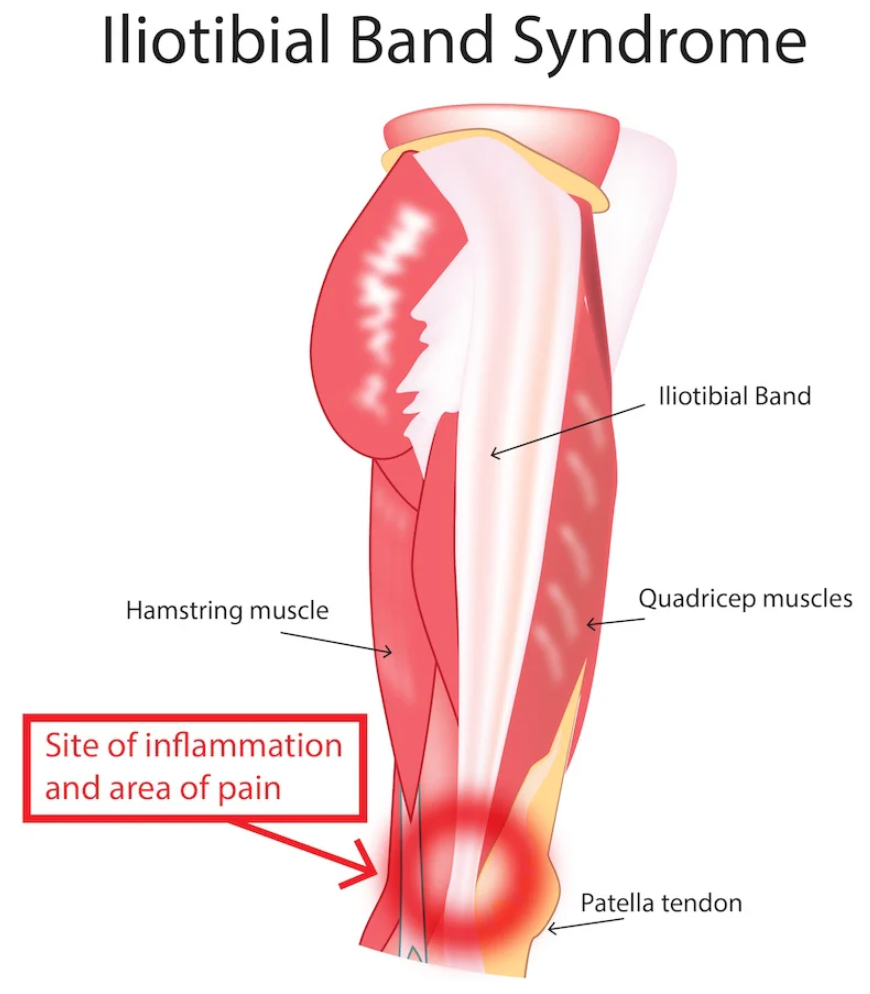
Anatomically, the ITB is an extension of the Gluteus Maximus (GMax) and Tensor Fascia Lata (TFL) muscles of the hip. (See image below) These muscles join together in a Y-formation just below the pelvis and continue down the outer thigh to attach just below the knee joint to a site on the Tibia (shin bone) called Gerdy’s Tubercle. The function of the ITB is to provide stability to the thigh and knee joint.
EVALUATION OF ITB SYNDROME
The evaluation of ITB Syndrome begins with an injury history of the athlete and standard biomechanical and orthopedic evaluation. Common findings include poor control/stability of the outer hip stabilizers (primarily Gluteus Medius), core musculature, and/or over pronation of the foot. Pain can often be elicited by pressing along the outer knee along the course of the ITB, but otherwise there are no specific problems detected at the knee.
When the Gluteus Medius is weak or inhibited, it does not keep the pelvis level with impact and/or loading such as during stance phase while running or pedaling while cycling. This allows the pelvis to dip on the opposite side. The body's response to this is to contract other muscles to compensate - in this case the GMax and TFL which end up tightening the ITB. As tension within the ITB increases, it puts pressure on the structures of the outer knee and causes pain. Also tied in with Gluteus Medius stability is muscular control of the core.
Muscular control of the core involves all of the muscles that wrap around the midsection of the body and extend down to the hips. When they contract they have a bracing affect.
To visualize this, think about how you would tighten your stomach muscles if you were to hit a tennis ball, throw a baseball, or cough. You should notice that muscles contract in a ring-like formation around your mid-section. Overpronation of the foot, as mentioned above, also ties into lower extremity biomechanics. Pronation is a normal phase of gait which allows the foot to conform to the ground as it contacts it during foot strike. Overpronation occurs when the foot rolls in too far in an uncontrolled way during foot strike.
TREATMENT OF ITB SYNDROME
As with most approaches in sports medicine, the treatment of ITB is individual and multifaceted. Treatment begins with symptomatic relief of the pain. This can be achieved with icing the knee to decrease pain and inflammation. Gel ice packs designed for sports injuries are the best and should be applied over top of a moist paper towel barrier. Ice no longer than 15 minutes per hour and remove the ice if it becomes too painful or once the area becomes numb. Icing should be limited to the initial phases of injury, as it’s use can prolong tissue healing.
The next aspect of treatment involves addressing soft tissue restrictions within the muscles, tendons. This is achieved by a number of soft tissue techniques such as Dynamic Motion Therapy (DMT), myofascial realease therapy, and instrument assisted soft tissue mobilization therapy (IASTM).
The goal of these therapies is to release excessive tension, scar tissue, and adhesions. When these restrictions are present in the soft tissue structures, they can cause pain as well as mechanically restrict motion patterns. Chiropractic manipulation and mobilization of the low back and pelvis has also shown to be effective to address pelvic rotations that result from muscle imbalance. Foot stabilization must also be addressed if that is a contributing issue. A running gait analysis is utilized to address biomechanical imbalances, determine shoe prescription, and it one aspect to determine the need for orthotics.
The final component of ITB Syndrome treatment involves exercise rehabilitation to restore the normal biomechanical stabilization. This helps to correct biomechanical imbalances and in doing so you will not only decrease your risk for injury but also improve your overall efficiency.
CONCLUSION
ITB syndrome is a common injury in endurance athletes, but it can also be seen in other sporting populations. Prevention starts with good biomechanics and proper core stabilization. Once injured, athletes can effectively be treated with specific soft tissue techniques, chiropractic manipulation, and exercise rehabilitation.